

An Expansile Mass of the Right Posterior Mandible
Case Challenge Number: 25
Diagnostic Introduction
History of Present Illness
The lesion was identified by the patient’s general dentist during a routine dental examination two weeks earlier. No pain, paresthesia, or other symptoms were associated with the enlargement. The patient denied any history of trauma, recent dental treatment, or previous oral lesions.
Past Medical History
The patient’s medical history was notable for hypertension, a benign thyroid lesion, and multiple spinal surgeries which she described as “fusions.” She also reported sensitivity to codeine. Her daily medications included condesartan cilexetil (32 mg) for hypertension, atorvastatin calcium (40 mg), and aspirin (81 mg).
Clinical Examination Findings
Extraoral examination showed no evidence of facial asymmetry or lymphadenopathy. Intraorally, a firm, expansile mass of the right retromolar area was noted. The swelling was more prominent lingually, although buccal expansion was also evident. (Figure 1) The overlying mucosa was intact and displayed a slightly bluish color. No palpable thrill was detected, and adjacent teeth were non-mobile.
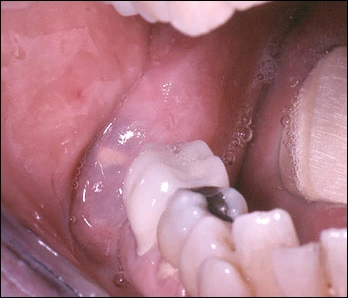
Figure 1. A somewhat lobular expansion with a bluish tinge is seen in the right retromolar area.
Radiographic Findings
The panoramic radiograph revealed a well-defined, 1.5 x 3.5 cm multilocular radiolucency involving the posterior mandible and the anterior aspect of the ascending ramus. Marked thinning of the superior portion of the posterior alveolar process and expansion of the soft tissue were also evident. (Figure 2)
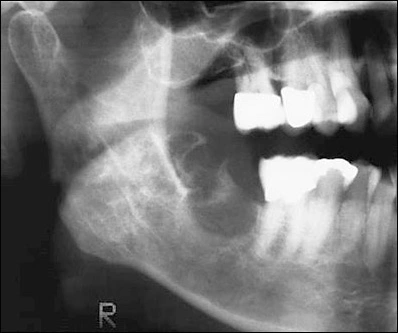
Figure 2. A relatively well-defined, multilocular radiolucency is noted in the right posterior mandible.
Computed tomography (CT) images showed significant expansion of both the lingual cortical plate (Figure 3) and posterior alveolar process. (Figure 4)
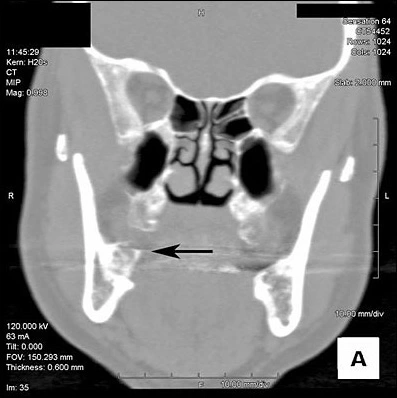
Figure 3. This cut of a coronal CT image shows a radiolucent, multilocular lesion with occlusal and lingual expansion of the right posterior alveolar process.
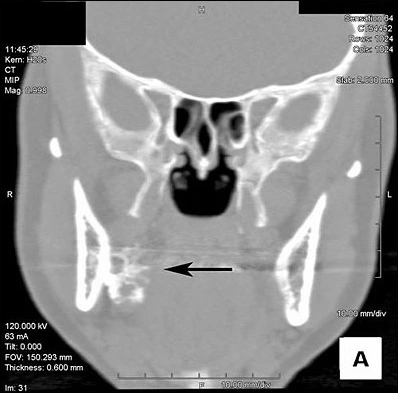
Figure 4. This cut of a coronal CT image shows prominent lingual extension of the lesion.
Unequivocal perforation of the cortical plates was not apparent, although the bone appeared markedly thinned. The internal aspect of the lesion had an irregular, mixed radiolucent/radiopaque appearance.
Histopathologic Findings
Microscopic examination of the biopsy specimen showed an unencapsulated neoplastic proliferation of squamous epithelial cells intermingled with plump basophilic cells containing foamy cytoplasm, consistent with mucin. (Figures 5 and 6)
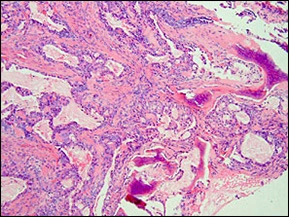
Figure 5. This low-power photomicrograph shows an unencapsulated proliferation of epithelial cells that are arranged in nests. (Hematoxylin and eosin)
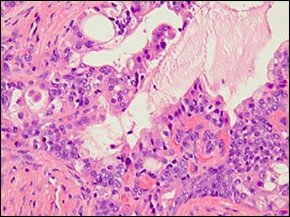
Figure 6. This high-power photomicrograph shows squamous and basaloid epithelial cells that sometimes form small cystic spaces. Scattered plump cells with pale, basophilic cytoplasm are also noted. (Hematoxylin and eosin)
The presence of small cystic spaces was also apparent. Histochemical tissue staining with the mucicarmine method demonstrated affinity of the cytoplasm of the basophilic cells for mucicarmine. (Figure 7)
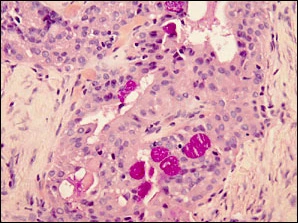
Figure 7. This high-power photomicrograph demonstrates the plump, basophilic cells have cytoplasmic affinity for mucicarmine, identified by themagenta-colored staining of these cells.